Submitted by Away-Pepper-9239 t3_11056fr in dataisbeautiful
Submitted by Away-Pepper-9239 t3_11056fr in dataisbeautiful
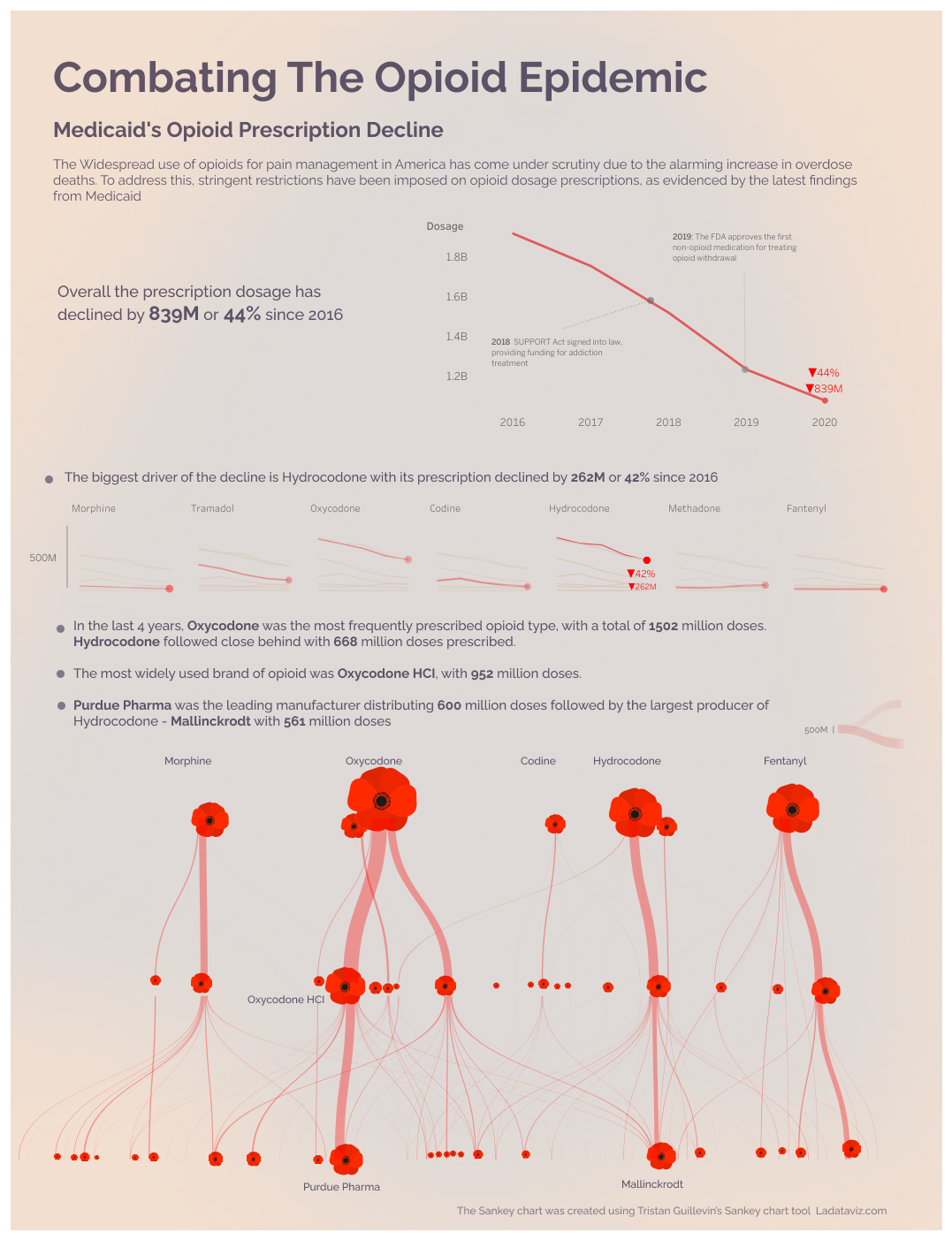
What a title! How on earth has prescribing less opioids considered “battling the opioid epidemic” when opioid use and overdoses are at all time highs?
This infographic depicts a pain epidemic if anything
This has everything to do with battling the opioid epidemic. Doctors were misled and lied to by Purdue reps regarding the addictiveness of these drugs. Purdue pushed oxycodone HARD. This absolutely led to patients becoming addicted, and later overdosing. Purdue was taken to court by multiple states over this.
Eh, doctors knew, every one has known that opioids are addictive for hundreds of years. Are the Sacklers scum? You bet, but let’s not put all the blame on them. Vicodin used to be prescribed for minor injuries, as a kid I remember getting codeine cough syrup every winter, people with chronic pain were perpetually prescribed dilaudid, and somehow I’m to believe the “opioid crisis” was caused by OxyContin?
Sounds like your mind is made up…
Can you refute anything I said? Or comment on the fact that opioid deaths and use are up even though prescriptions of opioids have become almost impossible to get for the last five or so years?
This data talks about the decline but not the increase of death due to illegal substances being laced on the streets. Also alot of individuals now go to the ER for an injection which has driven up the cost of medicaid and insurance.
Thanks, these are the nuances that a single dataset cannot depict thoroughly
[removed]
[removed]
You know there are painkillers besides opioids?
US consumes 80% of the worlds opiods. How is that "almost impossible".
Can you list them please
I thought that sounded like that number made about zero sense, and I found that the “80%” figure you mentioned has been repeated all over the place and it’s incredibly false. At one point in time, at one point, the United States had 80% of world’s sales for oxycodone. 99% for hydrocodone (every other country uses different stuff like classic morphine). Careful with statistic facts and numbers out there, I tend to remind myself constantly.
Oxycodone and Purdue is a problem that definitely should be talked about but if we hyper-focus on it too much we are missing about a hundred chapters of the rest of the story. Or twenty chapters, I don’t have an exact number but you know what I’m saying.
Pharmaceutical companies are the devil.
Red poppy’s are not opium poppy’s they are usually lighter in color
Yeah, but what else, if not opioids, I'm supposed to take when I see infographics like this?
Some non-opoid analgesics include: paracetamol NSAIDs e.g. ibuprofen, diclofenac, naproxen aspirin Ketamine Duloxetine (used for.neuropathic pain) Gabapentinoids such as gabapentin and pregabalin (also for.neuropathic pain) Local anaesthetics such as lidocaine, bupivacaine, ropivacaine (can be used in creams/gels/injections) Clonidine Magnesium Alcohol (studies have found it to be superior than paracetamol in certain quantities though obviously is also addictive!) Heat/cold therapies Steroids such as dexamethasone can provide some analgesic effect TENS machines Nitrous oxide
Many of these are situational e.g. if you have a deep pain than local anaesthetic cream likely won't penetrate deep enough, but a deep injection or nerve block of local anaesthic such as bupivacaine may work wonders.
There's gabapentin which is decent for nerve pain.
Then there's stuff you might take for minor aches and pains; aspirin, naproxen, acetominophen, ibuprofen.
Fot severe pain, opioids are far more effective than any of those.
This is a massive topic that has began to spread. Here is the UK we are trying to get a handle on it, though the start was a bit different. Opioid drugs became licensed for use for cancer pains and were able to be prescribed.for GPs. Overtime they began to be prescribed for other pains as well and as a result many patients got put on them for pains that thy wouldn't die from.
Unfortunately one issue is the opiod addiction that resulted, but actually, two other issues compound the problem massively.
Firstly over time patients develop tolerance. That is, the body essentially gets used to the opioid dose and needs more to have he same effect. What may have started with a pain needing 30mg of codeine a couple of times a day can progress over years to the same person needing 120 mg of morphine a day. GPs just kept raising he dose because that was often a.quicker/easier action than tackling the root problem. Chronic pain clinics are underfunded, have huge waiting lists and any success from them can take.weeks/months etc from the patient's initial consultation,.compared to a 15 second.raise in.the prescription dose.
Secondly, some.patients can develop opioid induced hyperalgesia. The pain pathways alter and thr opioid itself.can stimulate it causing pain. The patient is already.addicted to the drug and at this point the pain is chronic, so explaining that they need to reduce the dose is often met with refusal and disbelief (understandably).
Opioid can be very useful in the short term but long term they can be terrible.
Ah great, now people with surgically fused spines and cancer pain just get told "sorry bud, you can take some Tylenol?"
But I'm sure glad no one's abusing opioids anymore!
Yes. And sadly the damage is already done and will be until my generation is dead and gone. The war on drugs was a disguised war on the people....and opiates were the final blow that won it. More were lost from opiate overdose in it's worst year than the AIDS epidemic lost at it's height in the 80s. Where are the protesters looking for an answer to an end. Kissinger gave a model for population control...and boy are they using it.
UK here - coedine it the common drug here but hardly used in the states. How come? What is the difference
All poppys contain opiates.
But in significant numbers ?
But that would explain why people cut my poppy’s seed heads that are near a public road
No you’re right that opium poppies have the highest concentration, its just that all poppies have some level of narcotics in them.
I have had two back surgeries and I still have occasional severe pain in my lower back. I’ll ask for 4 or 5 Vicodin to get me through until it stops hurting. Usually takes about 3 or 4 days before the pain isnt debilitating. They act like I’ve asked them for crack and sex with their SO.
none of these treatments are effective against severe pain.
Good list but yeah very situational. Also I do not know if I am an outlier but unless I have swelling I do not take NSAIDs and acetaminophen has never done much in my experience. Maybe it helped with one headache in my life haha. Tylenol liver issues and NSAID issues but they make special formulas for longer term use now (coated to not harm GI).
Gabapentinoids maybe but it has its own side effects - might not be great for neurology long term like most things though I guess but might be more pronounced in a drug like pregabalin (neuroplasticity).
Clonodine and fluoxetine don’t seem very light either not to bash them if they work great for someone and they do not mind side effects.
Local anesthesia seems to have some serious draw backs from my quick read and makes sense why I haven’t heard of it more.
I’ve known someone who had back pain from like a pinched nerve in a herniated disk get a steroid shot that lasts a long time but I don’t know how many situations that can be applied to and what steroid side effects are like.
Alcohol seems a bit meh to suggest as chronic pain reliever and magnesium seems like a long shot but if it works I’m glad for those people. I do not use pain medicine or have had issues with chronic pain so I do not mean to bash the list but yeah we are in desperate need for drugs that produce analgesia or block pain like opioids do.
Wrong. If you have a foot amputated I can block the pain completely with a nerve block of just 20mls of local anaesthetic in the correct locations. Or I can give you ketamine and your pain is no longer an issue.
Similarly I know patients who cry out with their pains and they are on 160mg of morphine twice a day with extra opioid doses in between. Blatantly if they are crying out, the opioid are nit effective.
I've anaesthetised patients for operations, given them 20mg morphine and they are still in severe pain in recovery. Then you give them some IV paracetamol and diclofenac and the pain goes from 10/10 to them happy and chatting.
It all depends on the situation.
Correct in that it would be great if we had more drugs to choose from and yes, like all drugs they all have side effects, pros and cons and are situational. No drug is perfect.
Plus I listed analgesics because that is what someone asked for a list of but I didn't mean that all are suitable for chronic pain. Very little is. In fact the best therapies often aren't pharmaceutical for chronic pain.
R.e. steroid side effects they include increase in glucose levels, reduction in immune system response, a decrease in endogenous steroid production, increaser risk of GI bleeding and weight gain/hunger. Very unlikely to get these from a single injection like your friend though and actually it's unclear why single shot steroids remain so effective for as long as they sometimes do.
You’re good I was just looping it back into the conversation which is opioid replacements. And yes I only emphasize side effects because the drastic severities for example dementia later in life versus some tiny weight loss or gain.
Sorry to ask so much but we’re learning lots here.
Ketamine is a new one for me in terms of chronic pain. You remain conscious, like it’s a low dose?
I’ve never done intravenous acetaminophen plus an NSAID so I could see that being much better than oral potentially.
How often can you do nerve blocks and what’s the longest they last like half a day?
Ketamine is very variable in terms of side effects depending on the doses you use. I doubt it would be good for long term use but acutely it is awesome because it remains cardiovascular stable so it's great for trauma patients who have lost loads of blood, it's a bronchodilator so it's great for asthmatics and you don't have as much respiratory/airway loss like other anaesthetic induction agents. But that is all from a general anaesthetic dosing point of view.
At lower doses I've used it for dressing changes on burns patients and for manipulating kids dislocated limbs. You give a small dose, wait for them to go into a sort of fugue state and then pop the shoulder back in.
It is associated with the potential for profound hallucinations and increased salivation though. It provides a dissociated consciousness. One patient described it as like he was watching what we were doing to him as if it was like watching a TV show. No pain at all but it didn't feel real. Some hate that feeling, some don't care.
Again though I suspect long term use, which I am not familiar with,comes with side effects and problems.
Nerve blocks can last between a few hours and a full day. Depends on what you use, where it is used and how much. But it's labour intensive. Not really something that can be done every day. Plus there is alway the risk that the needle causes damage to the nerve if the person isn't careful with it.
A few places for chronic pain give IV lidocaine infusions. You come in for a few hours, get the infusion with monitoring. Then go home the next day. Again labour intensive and so often the funding isn't available to have it in many locations.
The best therapies in terms of long term benefits are usually physiotherapy and psychology. Ultimately if a pain becomes a chronic pain, the neural pathways alter and essentially don't work how they should do. Therefore removing the pain entirely often becomes impossible and those two therapies help the most because they help the patients accept and deal with the pain so they can get on with life. Unfortunately many patients are unwilling to accept this reality and believe there is a magic cure, a silver bullet, a perfect pill that sorts everything out.
Cool infographic! If I were you I’d definitely avoid using old-style figures alongside capital letters. The capital M in the second paragraph sticks out like a sore thumb and honestly I can’t unsee it. You could use a small cap M to make it more comfortable to the eye.
Also that whole paragraph just repeats information that is already clearly conveyed in the graph and it feels redundant. It would be more useful to use that space to make the graph bigger or replace that text with something that tells us information that we already don’t know by looking at the graph.
[deleted]
Many of these are not appropriate pain relievers for outpatient or chronic use. It’s like a person who doesn’t know anything about medicine wrote the post…
Firstly my post was simply a list of analgesics. That was what was asked for.
Secondly you may think that. And you are obviously entitled to your opinion. Your opinion is not seemingly well based in fact. Or perhaps maybe your reply is by someone who who doesn't know about outpatient or chronic pain use. I don't know.
I mention paracetamol, naproxen, ibuprofen, diclofenac, gabapentin, pregabalin, duloxetine, magnesium, local anaesthetics, heath and cold therapies, all of which are available and appropriate for some outpatient or chronic use. So basically the majority of what I listed.
You made a list of drugs that are not practical for most situations. It gives a totally misleading picture of the state of pain management as is related to opioid replacement.
I made a list of drugs for pain relief as that was what was asked for. There are very few situations (arguably none) in which all drugs are practical.
Expecting any drug to replace opioid is very unrealistic at this time and as I have commented on, dealing with chronic pains should be multidisciplinary and not entirely reliant on just pharmaceutical therapy for the most effective way of tackling the issue.
One of the largest barriers is tackling patient (and indeed many healthcare provider) mindsets and psychologies. Opioid rotation is not a long term solution. Opioid reduction is the main aim but requires a huge turnaround of thinking/effort/money.
Prevention is better than cure generally. Stopping the opioid problem in a patient beforenit deveoops into a massive chronic issue is far better than trying to sort it when they aren on 160mg BD and it's five years down the line. One situation that can be worked on is the acute pain apatient who comes to hospital (e.g. After a trauma). If the analgesia is effectively tackled then, with the likes of the medications I have mentioned, and they get discharged without the need for ever escalating opioid prescriptions, how is that a bad thing? If you disagree and you think they should just get ever escalating doses of single agents then, again, that's your opinion.
As of yet there is no panacea and I doubt there ever will be. Based on your name I'm guessing that you are somehow involved in the pharmaceutical industry? If this is the case then no doubt you are aware of how difficult it is to create a drug that has decent efficacy, acceptable tolerance and safety profile and a cost efficient process of manufacturing, distribution and marketing.
I never said
We literally use all of the drugs he listed for outpatient and inpatient management. In fact many of the post op patients now get High dose Ibuprofen, acetaminophen and Gabapentin as multi modal pain control as an alternative to opioids. I prescribe many of these daily.
Ketamine, alcohol, nitrous oxide… short acting injectable local anesthetic. None are reasonable for chronic pain management. Additionally the evidence for gabapentoids working outside neuropathy is extremely poor.
I didn’t say all were impractical, I said many.
…and high dose NSAIDs will end up killing more of your chronic pain patients than opioids.
Obviously multimodal is the way to go, but it’s also wrong to pretend we have easy, effective solutions for opioid replacement.
This is addressing prescription opiates, not street dtugs
This is addressing prescription opiates, not street drugs.
Until you need medication
I would argue that the movement to stop prescription opiates has made the opiate epidemic worse, not better, so shouldn’t be considered “combatting the opiate epidemic”.
It specifically says in the title "The Opioid Epidemic Medicaid's Opioid Prescription Decline" not all opiates
It's so sad that this is what the situation has become. Doctors are afraid of prescribing strong opioids for fear of being arrested. They can be abused for sure, but for some people with the most severe pain, it's the only way they can have a quality of life. It's leading some people to end their lives and nobody cares.
Thanks so much for the feedback. Will look out for capital M in the future and making the first paragraph more insightful
Do opioids actually help with anything?
It's cultivated for a reason.
"the prescription dosage has declined by 839M" What is this metric exactly? One "suggested serving size"?
Away-Pepper-9239 OP t1_j870l8r wrote
This is a submission to Tableau Health Project 2023. The data source was the Medicaid prescription data from 2016 - 2020
Check out the interactive link